UK GP Asthma Reviews Miss Spirometry Confirmation in Half of Diagnoses
Every year, millions of people in the UK carry a diagnosis of asthma. For many, the label is correct—and their inhalers keep them out of hospital. But for a substantial minority, that diagnosis may never have been properly confirmed. National audits consistently show that only about half of asthma diagnoses in primary care are backed by spirometry, the objective lung function test that guidelines recommend. The result is a system that both overdiagnoses and underdiagnoses, leaving some patients on unnecessary steroids while others miss treatment for conditions that mimic asthma.
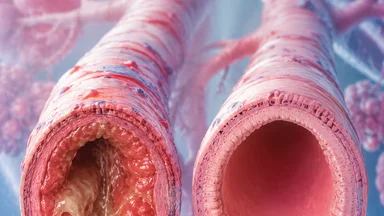
Half of UK asthma diagnoses lack spirometry confirmation
The National Institute for Health and Care Excellence (NICE) has recommended since 2017 that a diagnosis of asthma be confirmed with spirometry, ideally including a bronchodilator reversibility test. Yet repeated audits of GP records find that only 50–60% of patients labelled asthmatic have any spirometry result in their file. A 2023 analysis of over 200,000 records in England found that 47% of adults with a new asthma diagnosis had no record of spirometry within the preceding five years.
This diagnostic gap inflates prevalence estimates. Some researchers argue that true asthma prevalence in adults may be 30–40% lower than recorded figures. At the same time, underdiagnosis persists: a 2020 study in the British Journal of General Practice estimated that roughly one in five adults with objective evidence of asthma had never received the diagnosis. The net effect is a misallocation of resources—patients without asthma prescribed inhalers they do not need, and patients with asthma unrecognised until they present to emergency departments.
Primary care is widely cited as the main bottleneck. GPs see roughly 300 patients per 1,000 list size each year for respiratory symptoms, yet spirometry is often unavailable or impractical during a standard 10-minute appointment. The Quality and Outcomes Framework (QOF), which incentivises asthma reviews, does not require spirometry documentation, so practices have little financial motivation to invest in the equipment or training.
To illustrate the scale of the problem, consider a typical practice with 10,000 patients. If 8% of adults have a recorded asthma diagnosis, that is 800 patients. Among them, roughly 400 may never have had spirometry. If one-third of those do not truly have asthma, then about 130 patients are taking inhalers unnecessarily. At an average cost of inhaled corticosteroids of roughly £200–400 per patient per year, that practice could be wasting £26,000–52,000 annually on inappropriate prescribing. Meanwhile, the 130 patients with true asthma who are misdiagnosed as not having it may be experiencing preventable exacerbations and emergency visits.
Why spirometry is the diagnostic gold standard
Spirometry measures how much air a person can exhale and how quickly. The key metric is the ratio of forced expiratory volume in one second (FEV1) to forced vital capacity (FVC). In asthma, this ratio is typically reduced but normalises—or improves by more than 12% and 200 mL—after inhaling a bronchodilator. That reversibility distinguishes asthma from fixed airway obstruction in COPD, from restrictive lung diseases like pulmonary fibrosis, and from non-pulmonary causes of breathlessness such as deconditioning or anxiety.
Without spirometry, misdiagnosis rates exceed 30% in some studies. A 2018 systematic review found that among adults diagnosed with asthma in primary care, roughly one-third did not have asthma when tested objectively. The most common alternative diagnoses were COPD, vocal cord dysfunction, and gastro-oesophageal reflux. In older adults, asthma is frequently mistaken for heart failure, and the two conditions can coexist—making objective testing even more critical.
NICE guidelines also recommend spirometry for monitoring: the test should be repeated after a change in treatment or at least every five years. Yet follow-up spirometry is even rarer than initial testing. A 2022 audit of asthma reviews in London found that only 22% of patients had any repeat spirometry in the preceding three years. That means clinicians are adjusting therapy based on symptoms alone, which correlates only modestly with lung function.
The importance of objective testing was highlighted in a 2021 study from the University of Aberdeen, which followed 150 patients with a new diagnosis of asthma made without spirometry. After three years, 40% had been reclassified: 20% had COPD, 10% had bronchiectasis, 5% had heart failure, and 5% had no respiratory disease at all. Only 60% retained the asthma label. This reclassification led to changes in medication in nearly all cases, often reducing or stopping inhaled corticosteroids.
Clinical consequences of missed spirometry
The most direct consequence of a diagnosis made without spirometry is unnecessary treatment. Inhaled corticosteroids (ICS) are the mainstay of asthma control, but they carry dose-dependent risks: oral thrush, dysphonia, and at higher doses, an increased risk of pneumonia and adrenal suppression. Patients misdiagnosed with asthma may take these drugs for years without benefit, while the true cause of their symptoms goes unaddressed.
Delayed diagnosis of alternative conditions is equally concerning. COPD, for instance, is often diagnosed only after a patient has had symptoms for several years, by which time lung function may have declined substantially. A 2021 study in Thorax found that among patients over 40 with a new label of asthma, one in five actually had COPD on spirometry. Those patients would benefit from different bronchodilators and pulmonary rehabilitation, not ICS alone.
Vocal cord dysfunction (VCD) is another common mimic. It presents with wheeze and shortness of breath, often mislabelled as difficult-to-treat asthma. In a 2019 case series, 40% of patients referred to a specialist asthma clinic had VCD rather than asthma. Spirometry with flow-volume loop analysis can suggest VCD, but the test is rarely performed in primary care. The result is years of escalating asthma therapy that does not help.
Even when the diagnosis is correct, annual reviews that rely solely on symptom scores and peak flow diaries may miss deterioration. A 2020 study found that symptom-based control assessment had only 55% sensitivity for identifying patients with FEV1 below 80% predicted. Without spirometry, clinicians cannot distinguish poor control from fixed airflow limitation, and patients may be labelled as non-adherent when in fact their disease has progressed.
Beyond individual harm, there is a public health cost. Overdiagnosis inflates prevalence figures used for resource planning. If 30% of asthma diagnoses are incorrect, then the NHS may be over-allocating funds for asthma care while underfunding services for COPD, heart failure, and other conditions. A 2022 health economics analysis estimated that improving diagnostic accuracy in asthma could save the NHS roughly £200 million per year in reduced prescribing, fewer emergency visits, and better targeted care.
GP barriers to spirometry access
Why do GPs not perform spirometry more often? The barriers are well documented. Equipment cost is a factor: a desktop spirometer costs roughly £1,500–3,000, and calibration syringes add another £500. For a small practice with 5,000 patients, that may be a difficult upfront investment, especially when reimbursement is uncertain. Maintenance and infection control—cleaning mouthpieces, replacing filters—add ongoing costs.
Trained staff are another bottleneck. Spirometry requires a competent operator to coach patients through maximal effort and to recognise artefacts. The Association for Respiratory Technology and Physiology (ARTP) offers certification, but only a minority of practice nurses hold it. In a 2022 survey of English GP practices, 43% said they had no staff member trained to perform spirometry. Those that do have trained staff often report that the nurse is only available one day per week, leading to long waits for testing.
Time constraints during appointments are also a factor. A standard GP consultation is 10 minutes, insufficient for spirometry, which takes 15–20 minutes including coaching and repeat efforts. Some practices have tried nurse-led spirometry clinics, but these require dedicated space and appointment slots—resources that are scarce in underfunded practices.
Infection control concerns after COVID-19 further reduced spirometry rates. Many practices suspended lung function testing during the pandemic and have been slow to restart. A 2023 survey found that 30% of practices had not resumed routine spirometry, citing concerns about aerosol generation. Although guidelines now consider spirometry safe with appropriate precautions, the perception of risk persists.
There is also a cultural barrier: some clinicians believe that a careful history and response to treatment are sufficient for diagnosis. This view is at odds with evidence, but it persists. In a 2021 qualitative study of GPs in the Midlands, several expressed scepticism about spirometry, arguing that it is not always necessary in clear-cut cases. This attitude may reflect a lack of awareness of the misdiagnosis rates, or a pragmatic acceptance of resource constraints.
What the evidence says about alternative diagnostic tools
Given the barriers to spirometry, clinicians have looked for alternatives. Peak expiratory flow (PEF) diaries are widely used: patients measure their peak flow twice daily for two weeks and look for variability of more than 20%. However, PEF is effort-dependent and has low sensitivity—roughly 50% in some studies—meaning many patients with asthma will have normal variability. It also cannot distinguish asthma from COPD.
Fractional exhaled nitric oxide (FeNO) is a newer tool that measures airway inflammation. FeNO testing is quick, requires minimal coaching, and can be done in a few minutes. NICE approved FeNO as a diagnostic aid in 2014, but uptake has been slow. A 2024 survey found that only 12% of GP practices in England had a FeNO device. Cost is again a factor: a handheld FeNO monitor costs roughly £1,000, and consumables add to the expense. Reimbursement is also limited—FeNO is not included in QOF.
Questionnaires such as the Asthma Control Test (ACT) and the Asthma Quality of Life Questionnaire (AQLQ) are simple to administer but have poor diagnostic accuracy. A 2020 meta-analysis found that the ACT had a sensitivity of 65% and specificity of 72% for identifying uncontrolled asthma, meaning it misclassifies a substantial proportion of patients. For diagnosis, questionnaires alone miss up to 40% of true asthma cases, according to a 2018 study.
Portable spirometers have emerged as a potential solution. Devices like the NuvoAir Air Next and the MIR Spirobank connect to a smartphone and allow patients to perform spirometry at home. Pilot studies show good agreement with clinic spirometry, and patients find them easy to use. However, validation in diverse populations is limited, and the devices are not yet widely reimbursed. NICE acknowledged the potential of home spirometry in a 2024 update but stopped short of recommending it as a replacement for clinic testing.
Another emerging tool is oscillometry, which measures airway resistance using sound waves. It requires less patient effort than spirometry and may be easier to perform in young children or older adults. A 2023 trial in the UK found that oscillometry had comparable accuracy to spirometry for diagnosing asthma in primary care, but the equipment is even more expensive—roughly £5,000 per device—and training requirements are not yet standardised. As a result, oscillometry remains largely confined to specialist centres.
Three low-cost fixes that could close the gap
None of these barriers are insurmountable. Several low-cost interventions have been shown to improve spirometry rates in primary care. The first is nurse-led spirometry clinics. Primary care networks (PCNs) in England can pool resources to hire a respiratory nurse specialist who rotates between practices. A 2022 pilot in three PCNs in the North West of England increased spirometry coverage from 45% to 78% of asthma diagnoses over 18 months. The cost per practice was roughly £3,000 per year, offset by reduced prescribing of unnecessary inhalers.
Remote interpretation via telemedicine is another option. For rural practices where trained staff are scarce, spirometry tracings can be sent to a respiratory physiologist at a regional centre for review. A 2023 study in the Journal of Telemedicine and Telecare found that tele-spirometry had 92% agreement with in-person interpretation, and reduced the time to diagnosis by two weeks. The NHS England 2023–24 Improvement Scheme included funding for telemedicine in respiratory care, but uptake varied widely by region.
Mandatory spirometry documentation in QOF indicators would create a financial incentive for practices to close the gap. Currently, QOF rewards asthma review completion but does not require spirometry. A 2021 modelling study estimated that adding a spirometry indicator would increase testing rates by 25 percentage points over five years, at a net cost saving of £12 million per year due to reduced prescribing errors. The Royal College of General Practitioners has called for this change, but it has not yet been adopted.
Training programmes for healthcare assistants (HCAs) could also help. HCAs are already employed in most practices for tasks like blood pressure measurement and phlebotomy. A 2023 training programme in South London trained HCAs to perform spirometry in a two-day course, with ongoing remote supervision. After six months, 85% of HCAs were producing acceptable-quality spirometry traces, and patient satisfaction was high. The cost of training was £400 per HCA, a fraction of the cost of a specialist nurse.
A counter-argument to expanding spirometry is that it may increase workload without proportional benefit. Critics point out that spirometry is not perfect: it can produce false positives, especially in patients with normal lung function who do not show reversibility. However, this risk is lower than the risk of misdiagnosis without testing. Moreover, the alternative—relying on symptoms—has been shown to be even less accurate. A 2019 study found that clinical diagnosis alone had a positive predictive value of only 68% compared to spirometry, meaning nearly one in three positive diagnoses was wrong.
Another concern is that requiring spirometry for all patients could delay diagnosis in those who need immediate treatment. In practice, guidelines allow for a trial of treatment while awaiting spirometry, with the understanding that the diagnosis should be confirmed later. The issue is not that spirometry should be mandatory before any inhaler is prescribed, but that it should be performed within a reasonable timeframe—say, three months—to avoid long-term misclassification.
These solutions are not mutually exclusive. A combined approach—PCN-funded clinics, telemedicine support, QOF incentives, and HCA training—could substantially reduce the diagnostic gap. But they require investment and political will. In the context of a strained NHS, where primary care faces a workforce shortage and rising demand, even low-cost changes can be difficult to implement.
The evidence is clear: spirometry is the cornerstone of asthma diagnosis, and half of UK patients are not getting it. Closing that gap will not happen overnight, but the tools exist. What is needed is a recognition that the status quo—diagnosing asthma on symptoms alone—is no longer acceptable. Patients deserve a label they can trust, and clinicians deserve the tools to give them one.
This article is for informational purposes only and does not constitute professional medical advice. Always consult a qualified healthcare provider for diagnosis and treatment.